19 photos of hospitals before modern medicine
Step into a ward long before antibiotics and X-rays, and you’d find places that mixed shelter, charity, and treatment in unequal doses. In medieval Europe, big names like the Hôtel-Dieu in Paris or Santa Maria Nuova in Florence took in the sick alongside the poor and travelers. Meanwhile, in the Islamic world, bimaristans in cities such as Damascus, Cairo, and Baghdad organized care with separate wards and staffed pharmacies, setting an early benchmark for hospital administration and medical teaching.
These institutions weren’t clinics in the modern sense; they were social safety nets with beds. Care ranged from prayers and clean straw to bloodletting and broths. Wealthy patients usually avoided them, preferring physicians who visited at home. Hospitals served civic pride, piety, and public order as much as health, with endowments and city support keeping doors open. When epidemics hit, their roles swelled—and their limitations became painfully obvious.
Hospices, monasteries, and almshouses: where care began

Before the professional hospital, monasteries ran infirmaries where monks and laypeople could rest, be fed, and receive basic remedies. Hospices dotted pilgrimage routes like the Camino de Santiago, offering beds, soup, and spiritual comfort to footsore travelers. Almshouses sheltered the destitute elderly. Early London’s St. Bartholomew’s Hospital, founded in 1123 by Rahere, grew from a religious house that blended charity with basic nursing and occasional surgery—illustrating how sacred spaces slowly learned secular duties.
The lines between lodging, relief, and medicine were blurry on purpose. Founders wanted to save souls and bodies together, with chapels at the center of complexes and wards radiating outward. These places kept community rhythms: bells signaled prayers and mealtimes, and feast days meant special rations. Administration was a religious affair too—rules set by priors or confraternities governed who qualified for care, what they ate, and how long they could stay.
Charity over checkups: who got in and why

Admission often hinged on poverty, not a diagnosis. Many hospitals existed to serve the “deserving poor,” pilgrims, orphans, and foundlings. In 18th-century Britain’s voluntary hospitals, you frequently needed a subscriber’s recommendation letter to get a bed. Civic authorities and church officials prioritized cases seen as curable or pitiable. Chronic illness without prospects, or infectious disease during a scare, could mean rejection—or a detour to an isolation house instead of the main wards.
The well-to-do rarely checked in. They hired physicians to visit private homes, where rooms could be aired, linens laundered, and attention guaranteed. Hospitals were crowded and sometimes rough, and charity came with rules: patients swore not to beg while admitted, prayed at set hours, and agreed to discharge when ordered. That blend of moral screening and medical hope shaped who crossed the threshold and who remained outside, relying on neighbors and parish relief.
The smell of the ward: crowds, candles, and chamber pots

Picture a cavernous hall with rows of beds, low ceilings trapping heat, and windows cracked for whatever breeze would cooperate. Overcrowding was the rule in famous institutions like the Hôtel-Dieu, where reports described patients packed close together, sometimes two or more to a mattress. Lighting came from candles and oil lamps, which smoked, sputtered, and risked fire.
Add cooking smells from hospital kitchens, herbal poultices, unwashed wool, and it was a sensory onslaught.
Sanitation was a patchwork. Chamber pots tucked under beds filled quickly and were emptied on schedules that didn’t always keep up. Floors were strewn with rushes or scrubbed wooden planks, depending on the budget and era. Ventilation meant flinging windows wide or cracking dormer vents, even in winter. The better-run houses kept bedding aired in courtyards, whitewashed walls to cover grime, and posted rules about sweeping—small gestures against a persistent funk.
Beds were optional: sharing mattresses and space

Space was precious, and so were mattresses. In many hospitals, patients doubled up—or more—on straw-filled ticks or woolen pallets to stretch capacity and warmth. In a pinch, newcomers slept on benches, floors, or under beds until a spot opened. Sheets and blankets were valuable and thinly rationed; clean sets rotated slowly through washhouses, where boiling and drying took time. Bed curtains offered a semblance of privacy, though sounds and smells ignored the fabric entirely.
Sharing had consequences beyond awkwardness. Lice and fleas loved communal bedding, and respiratory infections traveled faster in tight quarters. Rules tried to sort patients by condition—surgical here, fevers there—but crowding often defeated intentions. Some hospitals placed mothers with infants together, the elderly together, and contagious cases apart when possible. Even so, the reality was compromise: a patchwork of bodies and blankets, each person hoping the mattress beneath them stayed dry and the neighbor didn’t cough.
Barber-surgeons and apothecaries: your care team, sort of
Hospital rosters mixed learned physicians, practical barber-surgeons, and busy apothecaries. Barber-surgeons handled the hands-on jobs—bloodletting, lancing abscesses, pulling teeth, setting bones—skills honed through apprenticeships and guilds. In London, the Company of Surgeons split from the barbers in 1745, reflecting surgery’s slow climb toward professional status. Apothecaries compounded remedies, dispensed simples and syrups, and in many places served as de facto general practitioners for those who could pay only a modest fee.
Physicians, trained in universities and fluent in Latin, consulted on complicated cases and prescribed regimens based on classical theory. They were few on the wards and many in private homes. Nurses, porters, and lay sisters kept everything moving: washing, feeding, sweeping, and steadying patients during procedures. It wasn’t a seamless team—guild rivalries and pecking orders mattered—but in a pinch, everyone’s hands were on deck, from shaving beards to mixing a mint infusion.
Theories that guided treatment: humors, miasma, and more

For centuries, medicine orbited the four humors—blood, phlegm, yellow bile, black bile—derived from Hippocrates and Galen. Illness meant imbalance, so treatments aimed to restore harmony with bloodletting, puking draughts, purgatives, and careful diets. Physicians read pulses, watched complexions, and recommended regimens of sleep, exercise, baths, and food tailored to a patient’s temperament. Astrology, seasonal cycles, and the doctrine of signatures sometimes nudged decisions, weaving culture into clinical choices.
By the early modern period, miasma—the belief that bad air spread disease—joined the rulebook. Hence the love of ventilation, vinegar fumes, and nosegays of herbs to ward off “corrupted” atmospheres. Contagion theories also circulated, especially during plague, arguing that people and objects could transmit illness. Without microscopes revealing microbes, debates stayed lively. In practice, a hospital might bleed a feverish patient, burn rosemary for the smell, and move the bed closer to a window—all bases covered.
Tools of the trade: leeches, lancets, and bleeding bowls

The instrument table would look familiar to a museum curator: brass lancets with tortoiseshell guards, folding fleams for opening veins, and cupping glasses warmed by flame to raise blood to the skin. Bleeding bowls, often ceramic or metal, were sometimes graduated to measure what was drawn. Apothecary benches held mortars and pestles, balances for weighing powders, and rows of jars labeled with Latin names for simples like digitalis, rhubarb, and opium preparations.
Leeches—Hirudo medicinalis—were kept in water-filled containers and applied to delicate areas where blades were risky. Enema syringes (clysters) stood ready for purges, while cautery irons waited in the brazier to seal vessels or destroy proud flesh. Splints and slings leaned by the wall; a bone saw and tenaculum lurked in the surgeon’s kit. None of it was sterile by modern standards, but it was practical, portable, and designed for speed and repeated use.
Surgery without anesthesia: grit your teeth and hold still
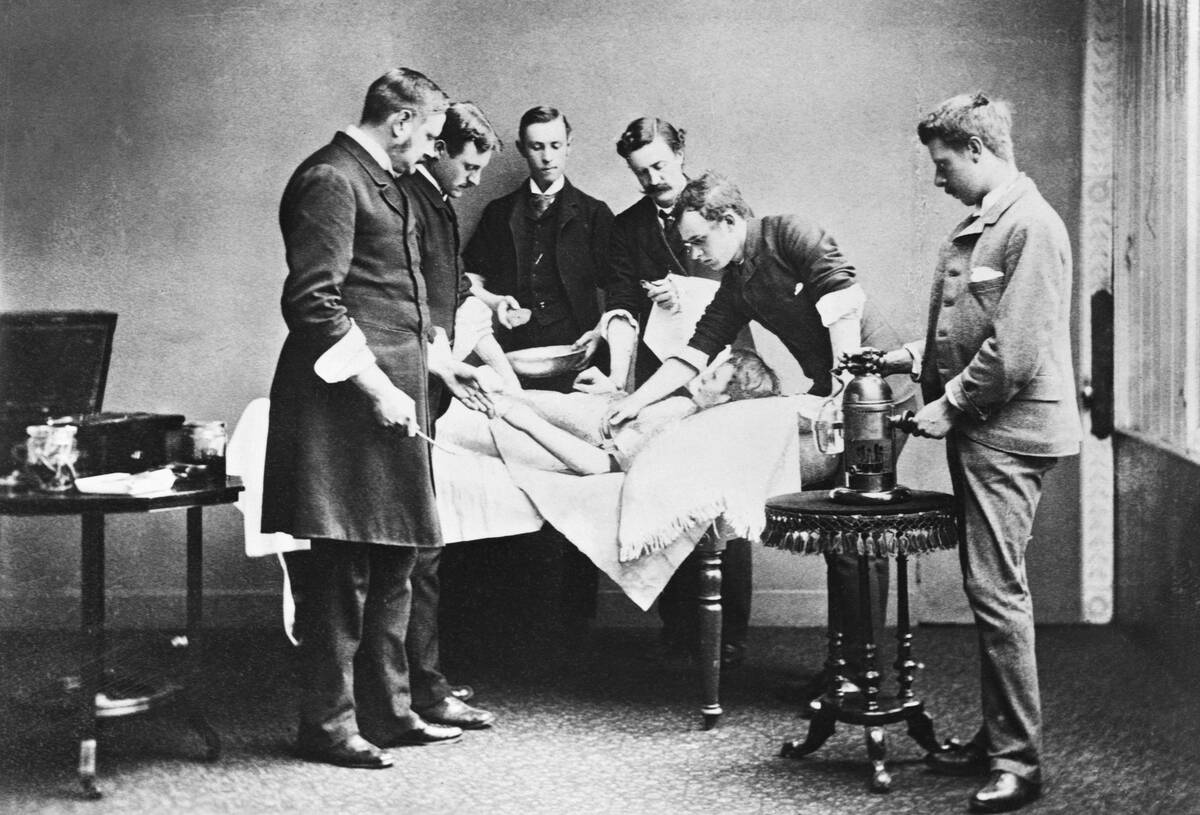
Before ether’s debut in 1846, “pain management” meant speed, strong arms, and whatever sedatives were on hand. Patients might receive alcohol, laudanum (an opium tincture), or mandrake-based concoctions, but full insensibility was rare. Surgeons trained to work fast—amputations measured in minutes—while assistants pinned shoulders and legs. A leather strap, folded cloth, or wooden stick gave jaws something to bite besides the tongue, and prayers provided the rhythm section.
Technique still mattered. Tourniquets squeezed arteries, and surgeons aimed for clean incisions, swift ligatures, and tight dressings. Reputation hinged on outcomes and spectacle. Names like Robert Liston became famous for speed and comparatively low mortality in a brutal era. Recovery took place in noisy wards where infection was a constant threat; opium might soften the edges, and cold compresses dulled throbbing. The bravest tool in the room, more often than not, belonged to the patient.
Fighting infection before germ theory: luck, limewash, and prayers
Without microbes to blame, hospitals fought “putrefaction” with what they could see and smell. Walls were whitewashed with lime to brighten and, people believed, purify. Vinegar and smoke were common deodorizers; some wards burned herbs or sprinkled chloride of lime as it became available. Linens were boiled and sun-dried when weather allowed, and surgical tools were wiped clean—though not sterile. Foul air was an enemy, so windows were prized and overcrowding, at least on paper, discouraged.
Staff leaned on routine: frequent sweeping, bedding aired in courtyards, and contaminated straw carted away. Fever wards, where they existed, tried to separate the very ill. Chaplains offered prayers, and processions or quarantines marked outbreaks. Despite this, wound infections, gangrene, and “hospital fevers” (often typhus) took grim tolls. Success sometimes looked like survival by luck and good ventilation, a patient discharged with scars, and a note to scrub harder next time.
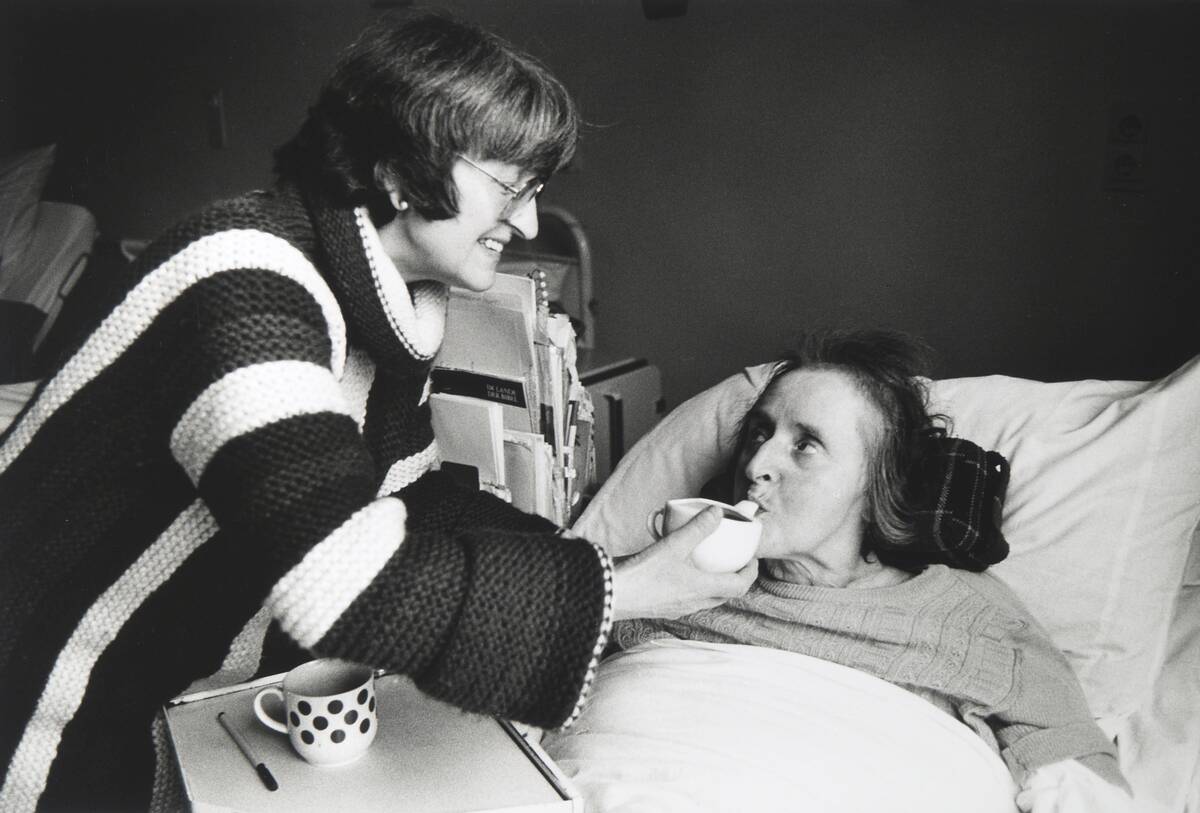
Nursing before Nightingale: nuns, neighbors, and “goodwives”

Long before formal nursing schools, care flowed from experience and vocation. Religious orders such as the Sisters of Charity in France staffed hospitals with discipline and daily rounds. In the Low Countries, beguines—laywomen in semi-monastic communities—ran hospices that blended piety with practical skill. Elsewhere, hospitals hired lay nurses, often widows or neighborhood “goodwives,” who knew how to wash, feed, and comfort the sick, and who learned dressings and poultices on the job.
Standards varied. Some institutions enforced strict rules—no drinking on duty, clean aprons, early prayers—while others tolerated rough edges in exchange for hard work. Compassion and cleanliness could be as influential as any prescription. The best nurses were prized for steady hands and sharp eyes, catching a failing pulse or a foul wound early. Pay was modest, room and board were common, and the hours were as long as the corridors.
Bring your own bandages: family caregivers at the bedside

Hospitals often relied on a patient’s inner circle. Families brought clean linens, shirts, caps, and sometimes the very bandages to wrap a wound. In many places, a relative or hired “watcher” stayed overnight to turn patients, fetch water, and keep fevers company. Personal items—rosaries, small icons, a favorite cup—traveled in bundles to make shared spaces feel less foreign and to soothe nerves when pain and noise made sleep a distant luxury.
This wasn’t just kindness; it was policy.
Some hospitals expected attendants to assist with feeding and changing, lightening the burden on thin staffs. Visitors might bring broth, soft bread, or fruit, especially when institutional rations ran plain. Rules tried to limit traffic during epidemics, but when gates reopened, families flowed back with the next pot of gruel. If you were lucky, a sister’s neat stitches or a neighbor’s patience made as much difference as any tincture.
Hospital food then: broths, beer, and bread

Menus were designed to be gentle and filling, not exciting. Broths, pottages, and thin stews dominated bowls, with bread as the dependable side. Meat appeared in small portions, more often for the recovering than the feverish, and religious calendars shaped what kitchens served. Many European hospitals issued rations of small beer or weak ale—the safer everyday drink when water sources were questionable—along with possets and milk-based drinks if a patient’s stomach could handle them.
Dietary rules could be surprisingly detailed. Some houses spelled out daily ounces of bread and beer; others reserved eggs or extra meat for the “most weak.” Kitchen gardens supplied leeks, herbs, and cabbages, while bakehouses turned out loaves by the dozen. Physicians tweaked diets by temperament—cooling foods for heat, warming for chill—fitting humoral logic to the pantry. A good cook, like a good nurse, was quietly therapeutic: steady, adaptable, and clean.
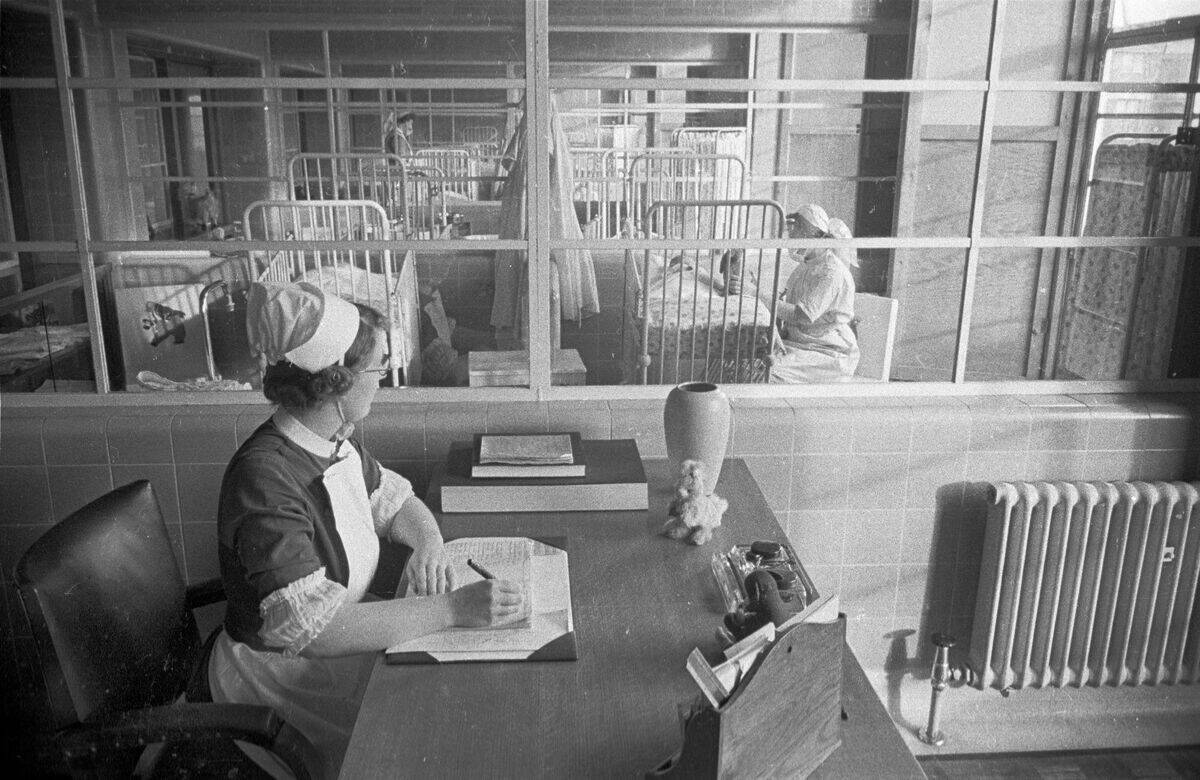
Record-keeping, if any: ledgers, letters, and memory
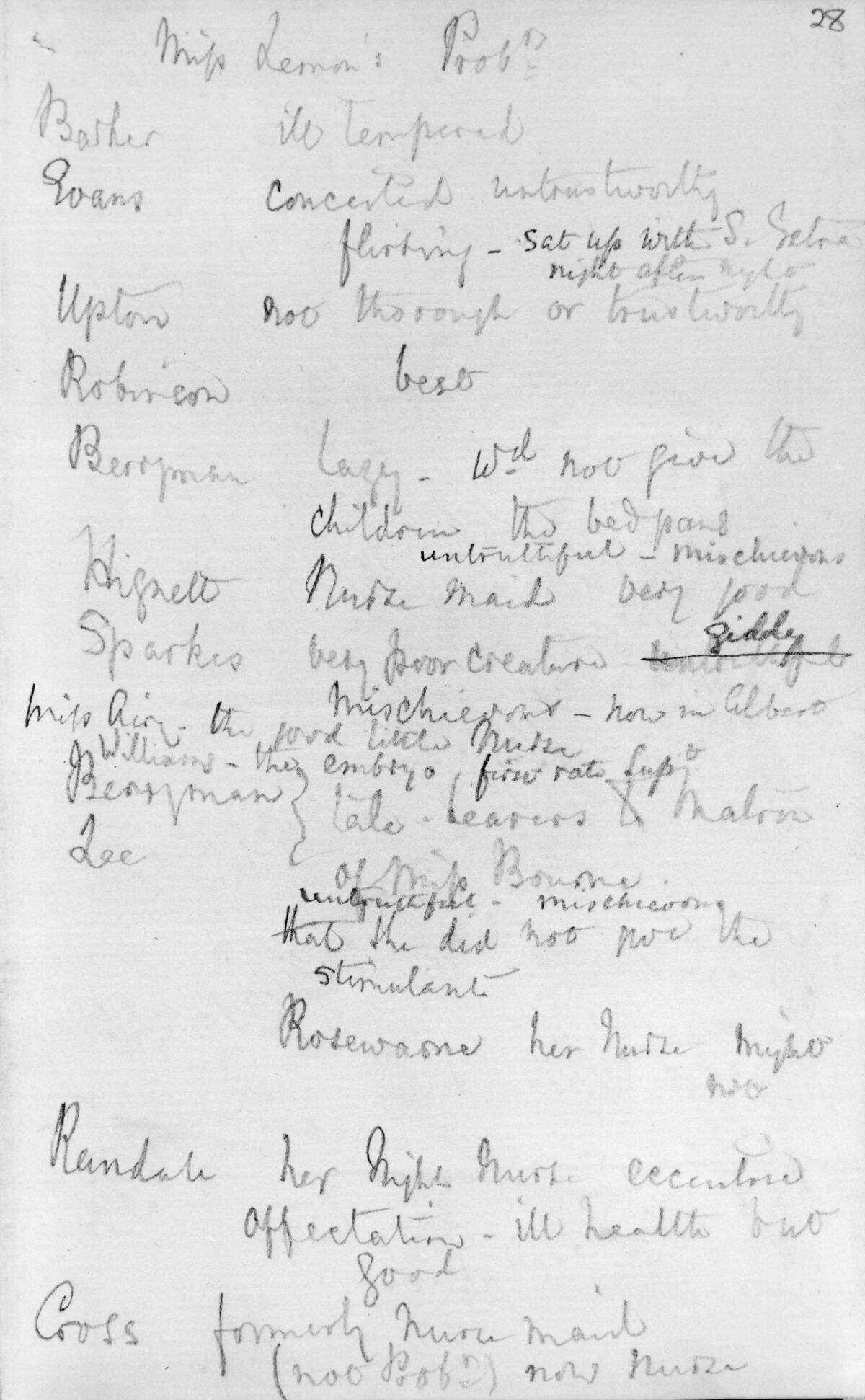
Paperwork existed, but it wasn’t a chart at the bedside. Hospitals kept ledgers of admissions, discharges, and donations; treasurers tracked endowments down to candles and soap. Patient-specific notes were sparse until the 18th and 19th centuries, when casebooks and ward journals grew more common. Earlier, a physician’s memory and a few lines in a personal notebook were the medical record, supplemented by the nurse who remembered who slept, who ate, and who didn’t.
Cities tracked sickness in broader strokes. Bills of mortality listed weekly burials by parish and cause—plague, pox, fever—offering crude trends that still shaped civic responses. Correspondence between doctors, or between hospitals and benefactors, sometimes mentioned striking cases or outcomes. Anatomy theaters kept registers of dissections, while poor-law overseers noted who needed relief after a long illness. It was enough to keep the doors open and lessons moving, if not to satisfy a modern auditor.
Isolation and pesthouses: handling plague and pox
When contagion loomed, cities leaned on isolation. Pesthouses sat on town edges to keep plague and smallpox away from dense streets. Port cities like Venice developed lazarettos—quarantine stations for ships and travelers—where forty days’ wait (a quaranta) tried to break chains of infection. Households under suspicion might be shut up, with guards at doors and marks warning passersby. Hospitals, anxious about spread, diverted fevers to these satellite sites whenever space and politics allowed.
Inside, care was basic: straw pallets, broths, and watchful eyes hoping rashes would crust and coughs would calm. Clothes were fumigated or burned; bedding was boiled; walls regularly whitewashed. Priests and ministers circulated for last rites, while surgeons lanced buboes when ordered. Mortality swung with the pathogen and season. When the crisis ebbed, cities argued—again—about funding permanent fever hospitals and how much quarantine was tolerable in the next emergency.
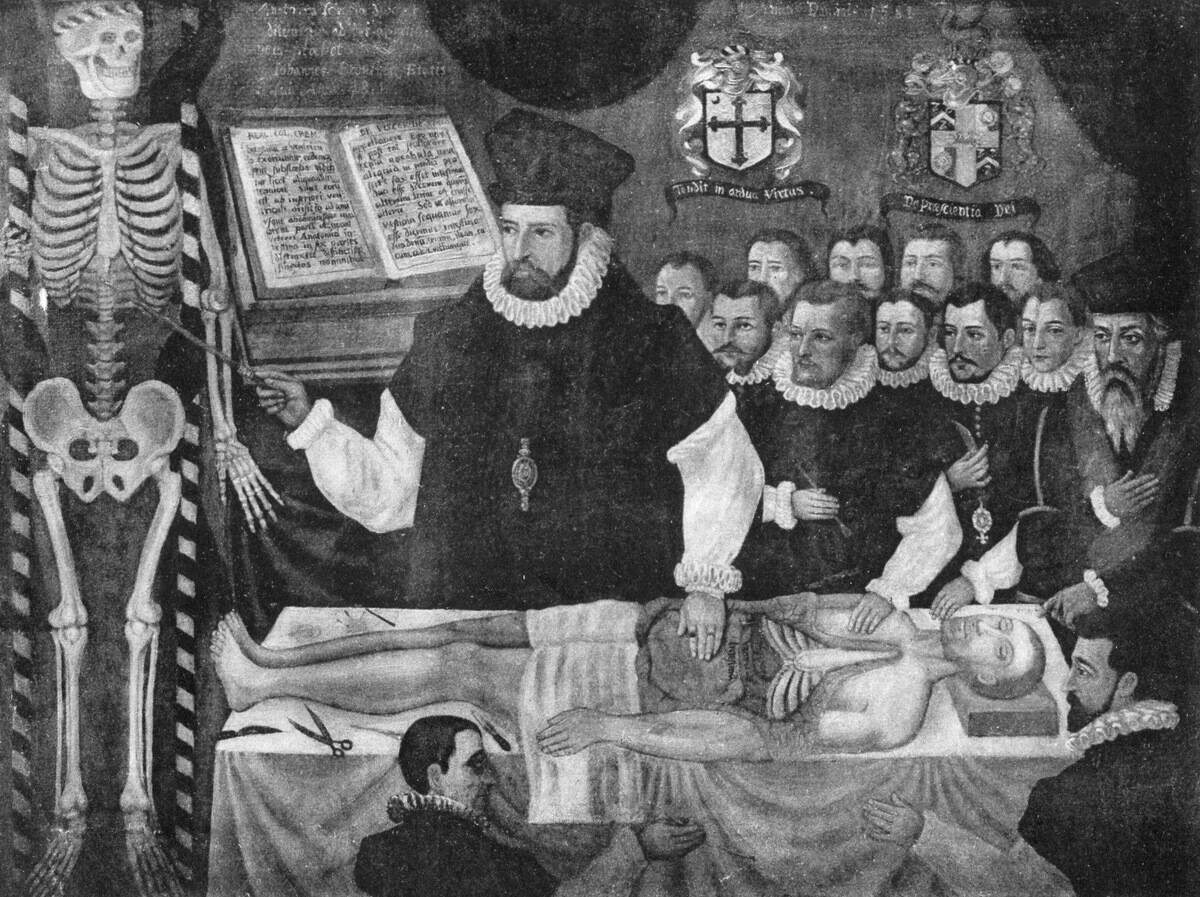
Teaching on the wards: public dissections and surgery theaters
Medicine learned in public. Anatomical theaters—like the famed ones at Padua and Leiden—hosted dissections as civic events, with students craning from steep galleries. Bodies, often of executed criminals per laws like Britain’s 1752 Murder Act, supplied anatomy lessons. Surgeons demonstrated operations on cadavers and, in some places, live patients, explaining technique and anatomy with brisk confidence while apprentices memorized each move and instrument.
By the 18th century, hospitals themselves became classrooms.
Clinical lectures at institutions in Edinburgh and London paired bedside observation with discussion of treatment and prognosis. Surgery theaters rose above operating tables so crowds could watch amputations or lithotomies. Notes taken in these sessions seeded the first systematic case histories. It was messy, loud, and illuminating—education built on proximity to suffering and the determination to turn experience into shared knowledge.
Asylums and “lunatic” hospitals: early mental health care

Institutions for the mentally ill ranged from grim to groundbreaking. London’s Bethlem Hospital—“Bedlam”—became synonymous with chaos, reflecting periods when restraint, spectacle, and poor conditions dominated. Treatments included purges, cold baths, and blistering plasters under theories that shocks could reset the body and mind. Families admitted relatives when home care failed or danger loomed, often navigating fees and rules that blurred charity with control.
Reformers offered alternatives.
The Quaker-run York Retreat, founded in 1796, pioneered “moral treatment”: calm surroundings, work, and respectful routines that reduced restraint. Later, physicians like John Conolly in England argued for non-restraint policies. Outcomes varied, but the shift mattered—compassion as a therapeutic tool. Even so, overcrowding and limited understanding meant asylums struggled, oscillating between humane ideals and the hard math of too many patients and too few attendants.
Military and battlefield hospitals: tents, triage, and trauma

War sped innovation by necessity. Field hospitals were tents, churches, and barns near the front, where surgeons worked through nights of cannon fire and shock. Dominique Jean Larrey, serving Napoleon, formalized triage—treating by urgency rather than rank—and developed flying ambulances to ferry the wounded faster. Amputations, bullet extractions, and ligatures crowded the docket, with tourniquets and bone saws earning every scar in the kit.
The deadliest enemies were often invisible: dysentery, typhus, and exposure.
Supply wagons struggled to keep lint, bandages, and opiates flowing. When weather cooperated, surgeons boiled instruments and water; when it didn’t, they wiped blades and pushed on. Recovery wards echoed with coughs and the clatter of tin cups. A soldier’s survival might hinge on where he fell on the line, whether a cart reached him quickly, and if the next tent had a free cot.
Money matters: endowments, guilds, and church support

Hospitals ran on charity and civic duty. Medieval founders endowed beds in exchange for prayers, while guilds and confraternities sponsored wards for their members. City governments chipped in when epidemics struck or pride demanded it. In Catholic regions, monastic orders and bishops steered resources; in Protestant cities, councils and trade groups filled gaps. Detailed account books tracked gifts of grain, candles, and coin, ensuring benefactors’ names lived on plaques and in prayers.
By the 18th century, Britain’s voluntary hospitals added subscriptions: donors paid yearly and received the privilege of recommending patients—a ticket to admission. Fees from paying patients, rental income from lands, and occasional royal favors rounded out budgets. Money shaped medicine: a well-endowed ward meant cleaner linens, more broth, and better lighting. A poor one meant stretched nurses and patched sheets. All of them chased sustainability with fund-raising dinners, sermons, and steady ledgers.
Early reforms and cleanliness crusades: the pre-modern push to improve
Even before microbes took center stage, reformers chased fresh air and order. In the 18th century, new fever hospitals and redesigned wards emphasized windows, cross-ventilation, and less crowding, echoing writings by figures like Sir John Pringle on cleanliness in military hospitals. Inspectors such as John Howard highlighted filth and infection in institutions, spurring whitewash, better bedding, and stricter rules. Quarantine systems in ports tightened paperwork and fumigation to keep contagion from stepping ashore.
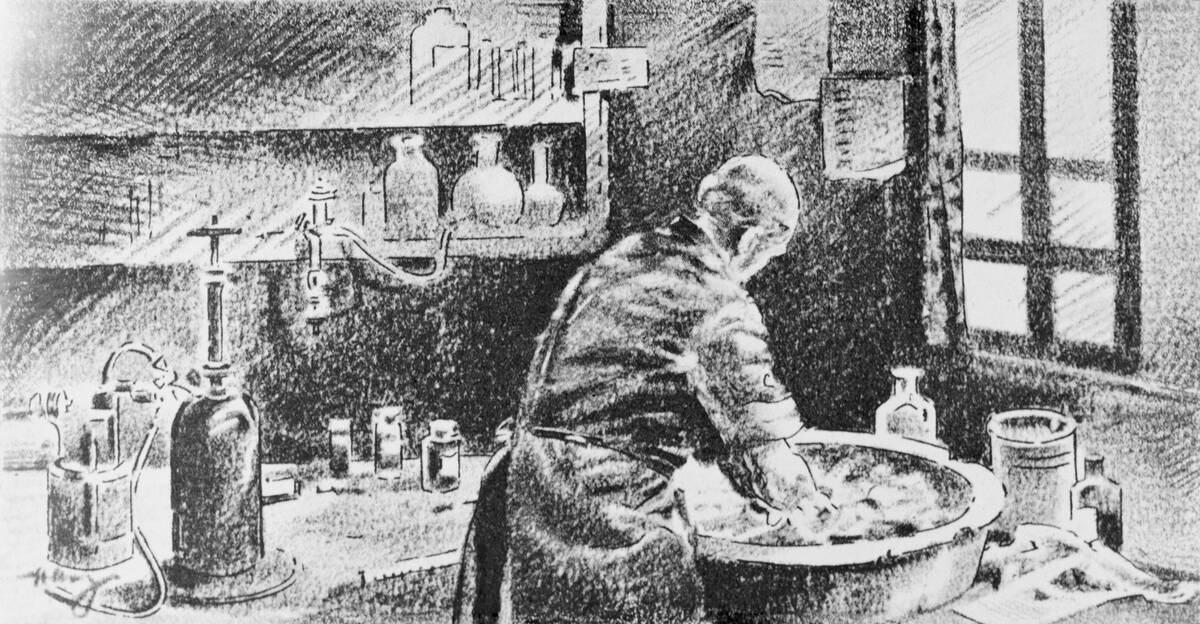
Handwashing had its champions too. In 1847, Ignaz Semmelweis cut puerperal fever dramatically by requiring chlorinated handwashing in a Vienna maternity clinic—years before germ theory won broad acceptance. Hospital bylaws increasingly banned bed-sharing, scheduled laundry, and insisted on airing wards daily. These weren’t cures, but they bent the curve: mortality dropped where ventilation improved and routines stuck. By the time antisepsis arrived, some hospitals already had the habit of scrubbing on their side.